The physiological and neurological effects of IQoro
IQoro exercises the muscles in the orofacial and swallowing processes from the lips, face, mouth, throat, upper airways and esophagus down to the diaphragm and stomach.
By closing your lips tightly against the handle and pulling the device forward, a low-pressure is created in the mouth making the tongue retract and seal against. The anterior palatal arch and the soft palate. IQoro flexes and trains the muscles and components along the swallowing chain, and they get stronger.
There are 148 muscles in the swallowing chain that are commanded and controlled by the efferent motor nerves. When certain of these muscles become dysfunctional the conditions that are treated by IQoro occur: drooling, poor facial control, poor postural control, dysphagia, Hiatal hernia, reflux, GERD, LPR, sleep apnoea, and more.
The physiological effects of IQoro training
In, for example, stroke survivors there may be damage to that part of the brain that was responsible for swallowing. IQoro training promotes the brain’s tendency to neuroplasticity: stimulating the previous pathways or assisting the brain to re-assign function to an undamaged area. This effect is seen when stroke patients regain their normal swallowing ability; and even when training starts years after the stroke event.
The neurological effects of IQoro training
Neurological processes are also triggered that cause the muscles to strengthen as IQoro stimulates the nerve pathways and the swallowing sensory-motor reflex arc. Inserting the IQoro pre-dentally immediately promotes stimulation of the lips, which is the vital first step. IQoro design includes scientifically, and specifically-designed and spaced, raised bumps on its outer face which target stimulation of the lips.
Four sensory Cranial Nerves (CN) are primarily involved. Stimulation of the CN Trigeminus (V) in the lips is the first step. In short order thereafter, the CN Glossopharyngeus (IX) and CN Vagus (X) nerves are also triggered, and then in turn the CN Facialis (XII) nerve too.
The training action of IQoro activates these four afferent nerve pathways with three ten-second bursts of intense sensory input. These nerves send powerful signals to the brainstem, and in turn the brain sends signals via the motor (efferent) nerves to command and control all 148 muscles involved in the swallowing process. This so-called sensory- motor reflex arc triggers involuntary, autonomic commands to the swallowing chain. Through all the touchpoints physically addressed, IQoro triggers afferent pathway activity to the Formatio Reticularis and the body’s natural swallowing process is thus brought in to action.
Not only swallowing is affected. The orofacial, respiratory, and swallowing processes and postural control are all indivisibly interlinked at the neurological level, where the Formatio Reticularis plays a central role in governing all the muscles involved in these functions. This is a key concept in understanding IQoro effectiveness – training with it exercises all these neurological pathways.
The three swallowing centres are triggered by the IQoro training action in the following sequence.
The first swallowing centre interprets the training action as that something is to be swallowed, and this instruction is sent to the second swallowing centre. The second swallowing centre transmits signals to the muscles via the motor nerves – the downward-transmitting efferent nerve pathways. Here, there is a pre-programmed ‘go/ no-go’ response: ‘swallow’ or ‘don’t swallow’ – a so-called stereotypical muscle response. When something is to be swallowed the command is sent first to the Nucleus Ambiguus (NA) an efferent nucleus which, in its turn, sends the instruction to swallow to the major components of the swallowing musculature via the motor, efferent nerve pathways. Concurrently, impulses are also sent to the third swallowing centre.
The five motor nerves that are important for swallowing are: CN Trigeminus (V), CN Facialis (VII), CN Glossopharyngeus (IX), CN Vagus (X) and CN Hypoglossus (XII). The first four are both sensory (afferent) and motor (efferent) nerve pathways.
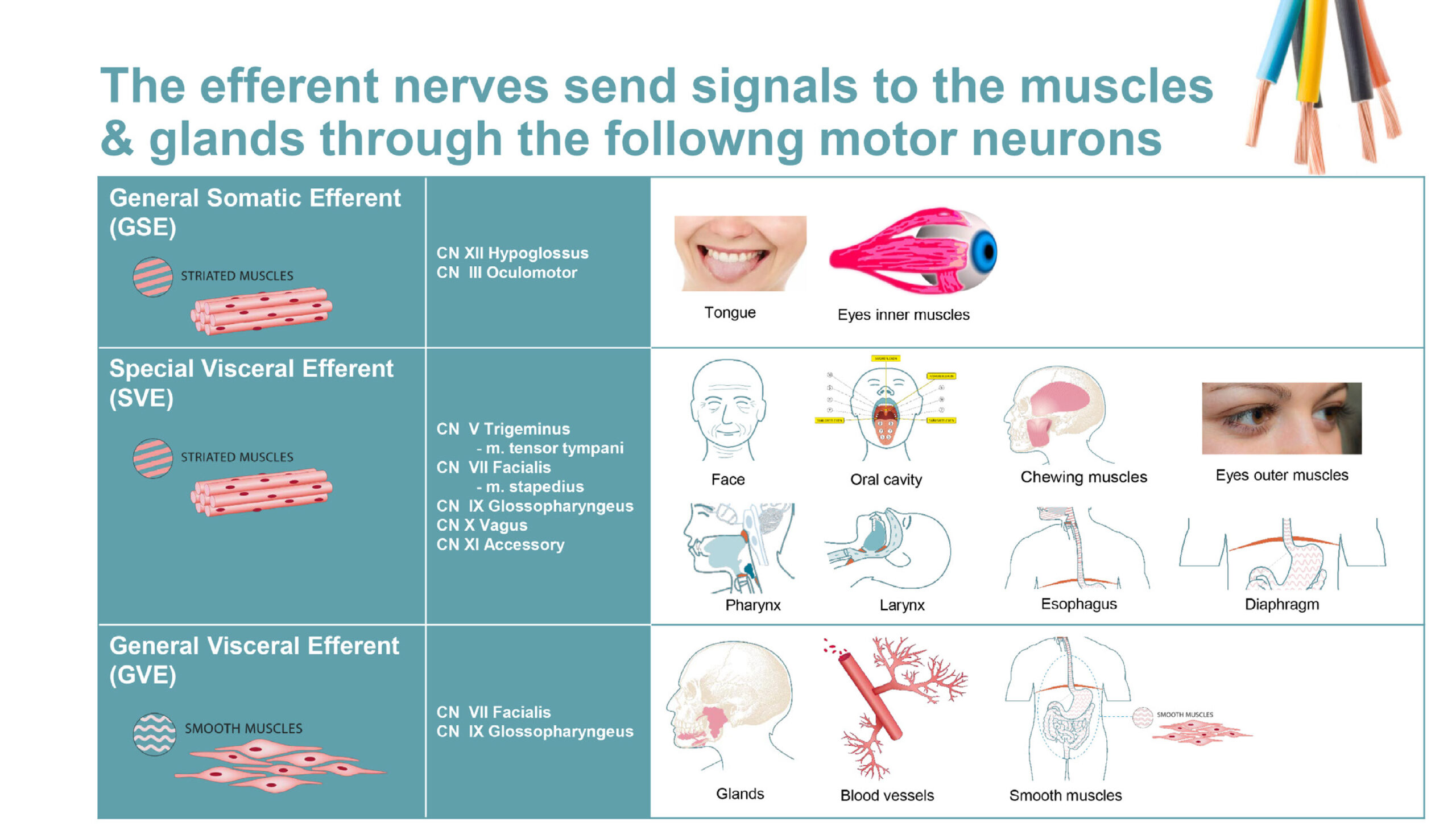
The third swallowing centre transmits information to the Nucleus Dorsalis Nervi Vagi (NDNV) an efferent nucleus, and then onwards to the esophagus’ musculature. The signals down to the muscles and glands are conducted via motor neurons in the brain stem. These nerves can be thought of as cables that contain various fibres, motor neurons, that conduct signals to the muscles and glands. In the brain stem there are three different kinds of motor neurons that are important in the act of swallowing. The General Somatic Efferent (GSE) motor neurones are present in the CN Hypoglossus (XII) and CN Oculomotorius (III) which transmit signals onwards to the tongue’s and the inner eyes’ voluntary skeletal striated muscles musculature. The Special Visceral Efferent (SVE) motor neurons act through the CN Trigeminus (V), CN Facialis (VII), CN Glossopharyngeus (IX), CN Vagus (X) and CN Accessorius (XI) which transmit signals to the voluntary musculature in the mouth, chewing muscles, facial musculature, pharynx, larynx, esophagus and diaphragm. The General Visceral Efferent (GVE) motor neurons act via CN Facialis (VII) and CN Glossopharyngeus (IX) which transmit signals to the glands, blood vessels and smooth muscles in the pharynx, stomach and rectum.
The signal pathways from the above-named motor neurons are: • CN Trigeminus (V) – signals via the SVE • CN Facialis (VII) – signals via the SVE and the GVE • CN Glossopharyngeus (IX) – signals via the SVE and the GVE • CN Vagus (X) – signals via the SVE • CN Hypoglossus (XII) – signals via the GSE
The sum of all the above signals set off a pre-programmed cooperation between the 148 muscles that are involved in the transport of each food bite from the mouth down to the stomach. The sensory-motor reflex arc promotes effective connections to the affected musculature, and the communication is rebuilt and strengthened. This manifests itself in improvement in swallowing, and then successively in other functions controlled by these circuits and executed by these muscles. Breathing and postural control function are stimulated and strengthened, as are the pharynx, tongue and soft palate, which accounts for the success of the IQoro treatment method in addressing snoring and sleep apnoea conditions. So, we have the two effects of IQoro on the muscles: one is both physiological and neurological (the upper muscle chain from the lips to the upper part of the esophagus) promoting movement, flexion and strengthening; and a second one, with only a neurological effect. The sensory-motor reflex arc re-initiates or redoubles its activity in stimulating the relevant muscles.
We might intuitively expect a case of muscle weakness caused only by physical factors, to be less complex than if caused by underlying neurological factors. (Compare for example a Hiatal hernia caused by strain, with swallowing difficulties caused by stroke). But in practice, it is usually the conditions with an underlying neurological cause that are successfully treated the fastest. This testifies to IQoro acting primarily on the neurological aspect. It also makes sense of our seeing a significant number of cases where a positive result has been achieved by an individual or a clinician after just a few days. This cannot be explained by increased muscle strength – even intense weight training in the gym has little effect in a few days. Instead, it is the improved brain motoric control that has been stimulated.
And, in a clinical study, IQoro was shown to be exactly equally effective in treating swallowing disorder and impaired postural control in a cohort that presented with both conditions. Some patients recovered from paralysis of the leg. Clearly, IQoro training had no physical effect on the muscles of the trunk, or the leg – rather the benefits were delivered via the neurological control systems that these two conditions share.
IQoro and Hiatus hernia
Here, we must reflect on another weakness of our ‘atrophied arm’ analogy. If we exercise our biceps and triceps we would expect them to build mass and strength; but we would be surprised if there were strength gains in other limbs that were not exercised directly.
In the case of IQoro training this parallel is not true, all the functions controlled by the neurological centres that we describe can be improved: including those not directly activated by the physical exercise.
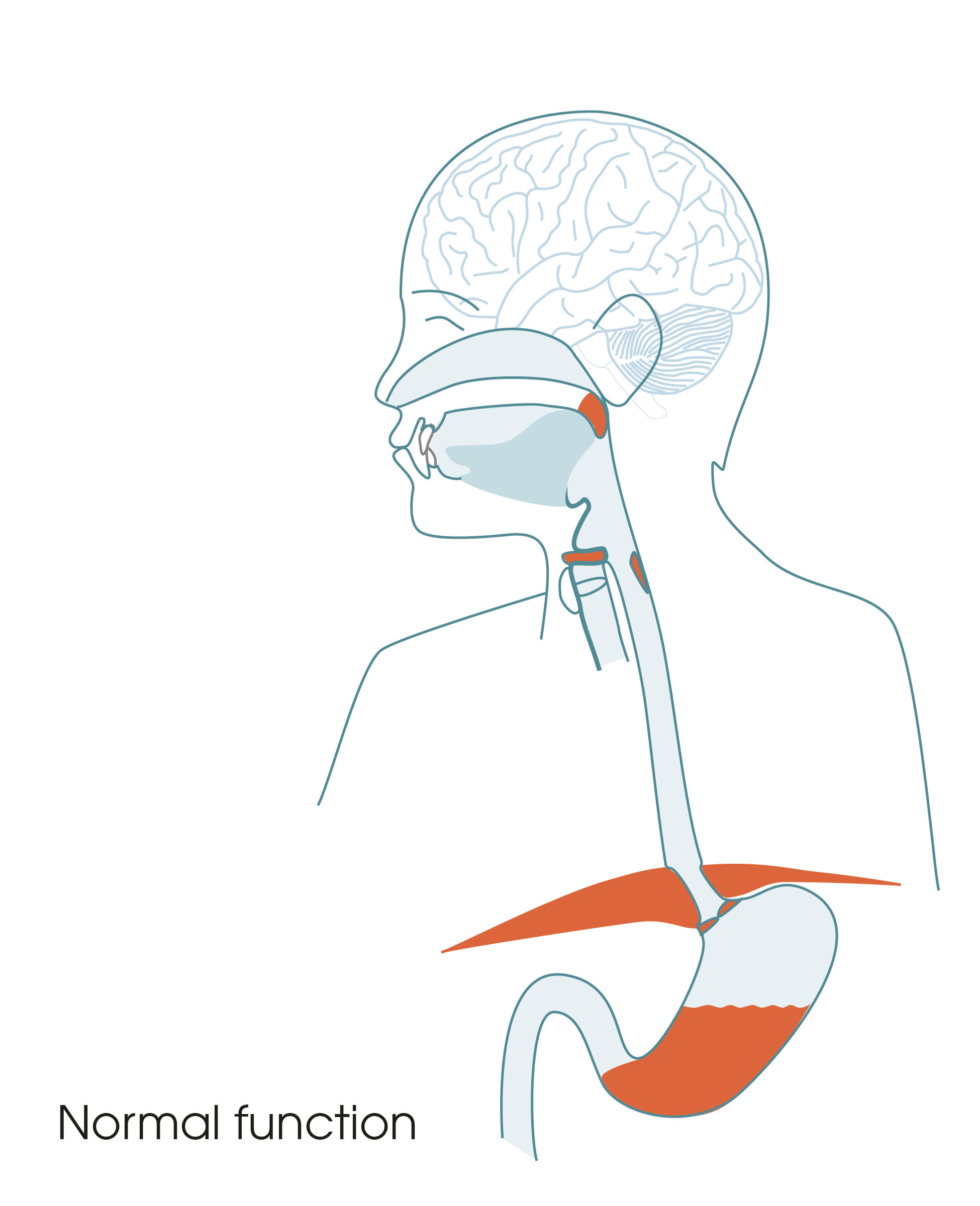
This effect is particularly evident when Mary and her research partners and students have explored what happens when IQoro treats a Hiatus hernia. There is evidence from clinical experience and high-resolution manometry, that the diaphragm is strengthened by IQoro training – repairing a tear or weakness in the diaphragm muscle.
A Hiatal hernia is a weakening or partial rupture in the musculature of the diaphragm. This rupture can allow part of the stomach and the Lower Esophageal Sphincter (LES) to slide up intermittently into the chest cavity and permit reflux of stomach liquids into the esophagus and beyond. This problem can manifest itself as heartburn, excessive saliva, thick phlegm, persistent dry or wet cough, a feeling of something stuck in the throat or behind the breastbone, gurgly or hoarse voice, etc. etc. This condition is often know as GERD (or GORD), LPR, reflux or silent reflux or other. It is known to increase the risk of other serious conditions too.

A Hiatal hernia can be the result of a neurological event like stroke or Acquired Brain Injury (ABI): the incidence of Hiatal hernia occurring or being aggravated after stroke is high. But it can also be purely mechanical: caused for example by pregnancy or lifting heavy weights, alternatively, insufficient chewing, or sedentary lifestyle can be the reason – no underlying neurological cause. The tear or rupture in the diaphragm muscle is outside the esophagus, so creating a partial vacuum in the esophagus cannot have a direct mechanical effect on the diaphragm muscle outside the hiatal canal. The long longitudinal muscles in the lower part of the esophagus are anchored under the diaphragm muscles and it can be the contraction of these long muscles that lead to the upper neck of the stomach being ‘pulled up’ through the diaphragm when the muscle there is weakened or ruptured. Physiologically this is the only potential direct physical connection IQoro training could have to the muscles of the diaphragm, and this is thought to be only a slight contributor to the treatment. Rather it is the sensory-motor reflex arc and the associated motor nerve pathways described above, that empower this natural neurological relay system, and the beneficial IQoro effect.
Conclusion
All can appreciate the effect of IQoro at a purely physical level – as a muscle exerciser – but this is less than half the story. Its greatest effect is in stimulating the body’s own pre- programmed natural neurological circuits and control.